
Report By Colin Wheeler
Almost all of my railway civil engineering experience was with British Railways before the unlamented Railtrack was formed. As a graduate I began “on the shovel” in an experienced city track maintenance gang and was “minded” by platelayer Charlie in safe track working. Later I learnt how to read track patroller’s reports and to listen and learn from maintenance gangers and Permanent Way Inspectors. Later still I met with the Division’s Chief Permanent Way Inspector whose practical views and opinions on trackwork were in many ways on a par with those of the relevant local divisional engineer.
After a short while, I could see that a depth of understanding from shovel level was complementary to engineering technical knowledge. Local experience together with that knowledge made the identification of faults and how to repair them easier. Record keeping was generally the job of “light duty men”; a benevolent euphemism for those knowledgeable trackmen retained in employment despite being unfit for manual trackwork, due to injuries sustained at work or age; or a combination of both! My early career began when “mechanised maintenance” (i.e., using rail mounted tamping, regulating and lining machines etc) was being introduced and track maintenance gang sizes and numbers were consequently being reduced as fewer men on shovels or ballast forks were needed.
Now we have the benefit of computing to store records and keep them available but have we lost many of the advantages of face to face listening together with sharing information and motivation with those whose boots are “ballast scratched”? Arguably this is evident from recent RAIB (Rail Accident Investigation Branch) reports and Network Rail’s Safety Central website.

Red, Green, Warning and Protection
Issued on 29 June on Network Rail’s Safety Central website was Local Safety Advice 21-01 from Network Rail’s “Project Manager Technical Authority”. It says that “Planners, Controllers of Site Safety (COSS’s) and other trackworkers will be aware that the terms Red and Green Zone working were removed from the Rule Book a number of years ago” and from 2017 from standard 019. Really?
The Advice adds that “Any text referring to Red and Green Zones that exists in the National Hazard Directory will be bulk updated to remove these terms on 30 June 2021”. It then asserts that the terms red and green zone will be replaced by “Warning SSOW” and “Protection SSOW” respectively; please check as I may have them the wrong way round! (SSOW Safe System of Work).
Newhouse Barton Western Safety Bulletin
Unauthorised Open Line Working with a three second near miss! On 21 June two trackworkers were patrolling in the four-foot on a curve and checking rail temperatures. Their sighting distance was inadequate when that moved to a place of safety with three seconds to spare before a train passed them.
The plan was for the work to be done using a “line blockage with additional protection”. The protection was refused by the Green Zone Access Controller! (Does the Technical Authority know they still exist?)
The planner did not know how to escalate the matter so the Safe Work Pack (SWP) was not amended before being authorised and issued to the PIC (Person in Charge). Poor mobile phone reception meant that the two were unable to contact the signaller to arrange protection so they continued their work without having a SSOW in place.
Hopefully the author of the Bulletin, Western’s principal construction manager will suggest that ease of understanding and simplicity are key on a day-to-day basis, and those changing rules and the Hazard Directory ought to get their boots well scratched by track ballast!
RAIB’s investigation of Roade track worker fatality
On 9 June the Rail Accident Investigation Branch (RAIB) published report 03/2021 following their investigation of the fatal accident to a trackworker who was struck by a train at Roade in Northamptonshire on 8 April last year.
The report summary is clear and concise, “the accident happened because the trackworker, who was the person in charge of the work with responsibilities as Controller of Site Safety, was walking along a line that was open to traffic and did not look back towards the approaching train on hearing its warning horn.
He had gone back onto track after handing back a blockage of the line, which had been taken to isolate the overhead line equipment, a task which it was later appreciated did not need to be done every day.”
Inadequate management systems and work planning
The investigation found that “performance monitoring and appraisal arrangements for the track worker were inadequate and did not identify and address issues of compliance with rules standards and procedures”. The system of work was inadequate for the work being undertaken and did not specify adequate arrangements encouraging compliance.
The report suggests that this possibly affected the behaviour of the trackworker and others. The report makes three recommendations, two for the employer AmcoGiffen and one for Network Rail. AmcoGiffen should develop and implement formal performance monitoring and appraisals for identifying and developing the ongoing safety performance and competence of its workforce at all grades.
Secondly AmcoGiffen should review management arrangements and resources to ensure that work is planned, undertaken and reviewed in compliance with its management systems, particularly in the early stages of establishing new projects and sites of work.
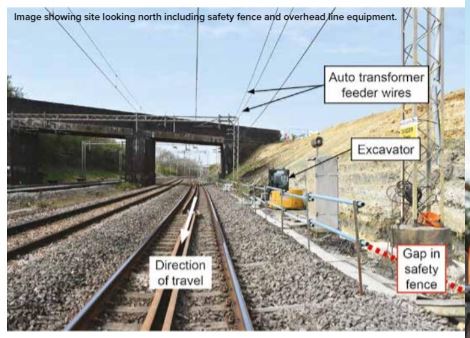
Remotely operated earthing devices needed!
The recommendations for Network Rail are far reaching. They are to review and amend their Electrical Safety Delivery programme to confirm that it takes account of the learning from the Roade investigation and consider ways of minimising the need for personnel to access the track, such as remotely operated earthing devices, and improved coordination and visibility of key information when planning and taking isolations of electrical supply and contact systems.
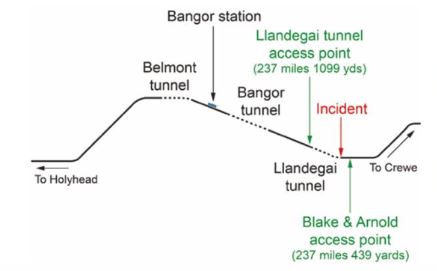
Llandegai Tunnel, Gwynedd near miss
On 30 June RAIB published their safety digest about a near miss on 13 February this year. It happened around 1233. The track worker was one of a group of two inspecting ice accumulation in the tunnel. His colleague was acting as “protection controller” and took a line blockage of the up line (eastwards) through all three tunnels.
After confirming that the up line was blocked, the protection controller became the Controller of Site Safety (COSS) and the two worked together. The approaching Shrewsbury to Holyhead train was travelling at close to its maximum speed of 75 mph when its driver saw the workers and sounded the horn.
One second to spare
The pair had entered the tunnel on the down line (used by westbound trains) and were using a long pole to remove icicles from the tunnel roof. Hearing the horn and seeing the train the COSS shouted that they were on the wrong line.
He managed to get to the safety of the adjacent line; the other track worker fell over, but managed to roll into the space between the two tracks. The train driver applied the emergency brake and again sounded the horn. CCTV shows the second worker rolled clear with just one second to spare.
No staff available
Both trackworkers worked for AmcoGriffen and managed a team contracted by Network Rail to carry out minor works on structures in North Wales. They could be called to check tunnels with ventilation shafts and deal with ice. Network Rail’s plan in Wales for dealing with the ice risk in tunnels is for trains to be cautioned when a “red warning” low temperature alert (72 hours of temperatures below zero degrees C) is experienced. It had been cold for several days and other AmcoGriffen staff had been deployed to tunnels across North Wales on 10 February.
The senior asset engineer and control were concerned and wanted to avoid cautioning trains. They arranged a reinspection of the tunnels to be completed before 2130 on Saturday 13 February. The engineer called the rostered COSS, who having no staff available, agreed with his manager that they would inspect the tunnels themselves.
Icicles and access points
Due to a driver’s report of icicles, trains were being cautioned through Penmaenbach tunnel near Conwy. The two travelled in separate road vehicles to Penmaenbach where they completed their work by 1130 leaving three more that were nearer Bangor.
One trackworker had been to Llangedai Tunnel before during a possession in 2019 so the COSS followed him to the access point used previously. The COSS spoke with Bangor signaller saying he was “at the Llangedai access gate” and needed 10-20 minutes to inspect the tunnel.
He was offered the up line for nearly an hour but told the down line would have to stay open. The COSS though this would suffice for all three tunnels so the relevant forms were completed.

Wrong access point!
The COSS referred to an access point list from Network Rail’s Hazard Directory, picking out “Llangedai Tunnel” where the track adjacent to the access was the up. They were actually at “Blake and Arnold” access point where the nearest track was the down line that was open for traffic!
This was the access used back in 2019. Consequently, they entered the tunnel on the down line from the wrong direction believing they were protected. Neither of them had been to the Llangedai access before. RAIB reviewed the 13 February train service pattern.
Had they waited a further ten minutes for the train to pass, another would not have been due for over an hour. The Blake and Arnold access point did not have a sign indicating which track was which.
North London Bell Isle Junction MEWP runaway
RAIB are investigating the runaway at around 3-40 am on the morning of 16 May of a MEWP (mobile elevated work platform) that occurred as it was being on-tracked.
A similar event happened in 2016. It ran away for about 700 metres on a 1 in 28 gradient in the direction of London St Pancras station. RAIB’s preliminary examination revealed that its direct wheel braking system was not correctly set for operational use and this was the likely cause.
The braking system, machine maintenance, effective braking, technical issue reporting and underlying factors are all being investigated.
Signal passed at danger Sileby Junction Leicestershire
On 5 May at 5-29 am a rail grinding/profiling train on the Down Slow passed a signal at danger by 350 metres stopping foul of the junction over which a train of empty coaches travelling in the opposite direction had passed less than ten seconds earlier! RAIB’s preliminary examination found no faults in the trains or signalling equipment.
Brakes on the grinding train were applied and the Train Protection Warning System (TPWS) intervened but the train did not stop within the safe overrun distance. RAIB are considering management of the train driver’s competence, signalling design Leicester/Loughborough, effectiveness of the TPWS and relevant underlying factors.
Safety Central MEWP basket contacted live overhead line equipment
On 14 May at 0038 at Wolverton on the West Coast Main Line south a technician was working in the basket of a Mobile Elevated Work Platform (MEWP) when it came into contact with live overhead line equipment (OLE). He was still in hospital with serious injuries on 18 May. The operator of the MEWP also sustained a minor injury. The work being undertaken was “routine planned OLE adjustments”. Both British Transport Police and the Office of Rail and Road are now involved.
Derailment risk following engineering work
At Barnehurst in Kent possession was given up around an engineering train which then left the worksite. Its driver on seeing an obstruction across the adjacent line spoke to the signaller who blocked that line. Two sleepers were chained and padlocked to the running rails. It has been established that the sleepers were left to create a barrier to control the risk of a “rail mounted plant runaway” leaving the site of work. I wonder if their use was specified in the SSOW?

Currently we have a sophisticated, computerised planning system to be proud of, but it contains some rules etc even in the Hazard Directory which are not accepted by those directly involved in doing the work. Without the buy-in and ownership of each safe system of work plan by the workforce and each and every shift supervisor the plan is worthless and potentially dangerous.
I recall using a system where technical staff and supervisors, who would be doing shifts together visited every site in daylight and agreed or if necessary, amended the working details so that they were committed to the detailed work method of every shift. Consequently, they carried out the work as planned. They both wore ballast scratched boots and were aware that if it all went wrong, they would suffer the consequences and get the blame!!
