
Individuals and teams make mistakes – it’s a fact of life. But I believe vertical slice audits and unannounced safety visits would help to prevent them. I also recommend that management regularly sits down and listens to those who do the work – human factors are important for all.
Trapped and dragged incident on Manchester Metrolink
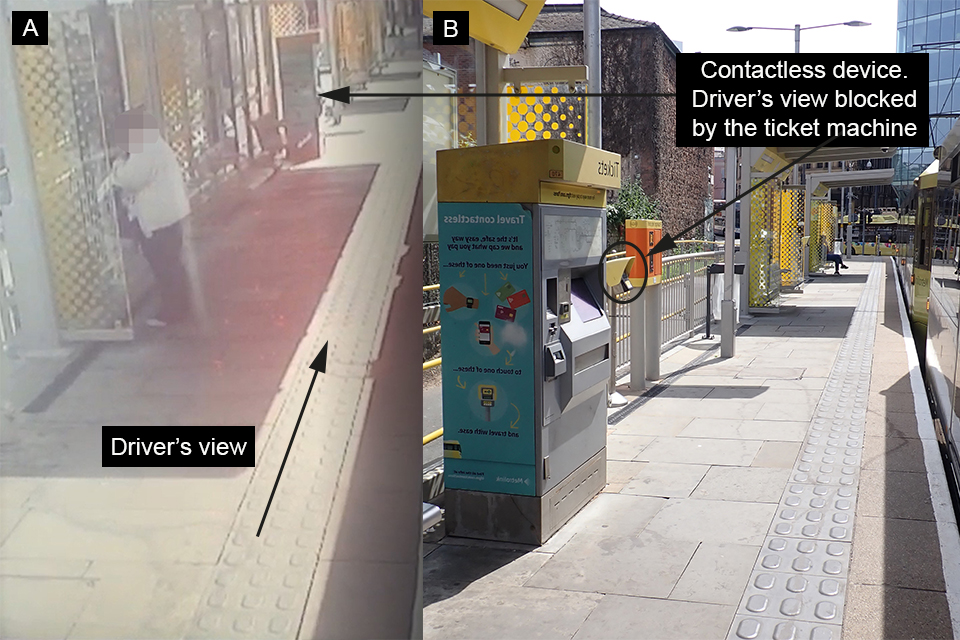
On 20 September, the Rail Accident Investigation Branch (RAIB) published Safety Digest 04/2022 about an incident that occurred at 11:17 on the morning of 27 May, where a passenger’s bag became trapped in the doors of a departing tram, trapping their hand. The incident, which occurred at Shudehill Tram Stop in Manchester, shared similarities with a number of previous incidents. As the tram arrived the passenger was walking along the platform with a companion and used a contact “touch in” device adjacent to the ticket vending machine. After touching in, the passenger started boarding as the doors began to close but then stepped back. The passenger’s bag was trapped with their hand caught in its strap.
The tram driver checked that the green “doors closed” light was illuminated and then started to drive away. The passenger was dragged for 13 metres before extricating their trapped hand and falling onto the platform. The tram driver was focused on a tram signal, and the pedestrians and vehicles in the road ahead. The driver was unaware of the incident until subsequently told about it by the Metrolink Operator. The Digest says that the cause was the driver failing to complete the final safety check before moving the tram away from the stop. “Consequently, the driver was unaware that the passenger was in an unsafe position when they decided it was safe for the tram to depart.”
The drivers’ Rulebook requires three checks using the tram’s CCTV system before the doors are closed to make sure the doors are clear before starting off. Once doors are closed, a second check using CCTV is intended to look for “trapped passengers or objects”.
Once satisfied, the tram driver may turn the selector switch to “drive”. The CCTV selector allows the driver to display either side of the tram, and images of the platform, from front and rear cameras similar to those provided by road vehicle wing mirrors. The Rule Book mandates a third check before the tram moves off to ensure nothing is trapped. The interlock system is designed to automatically reopen if objects of 30mm or more are detected. If objects less than 30mm are trapped, such as coats or bag straps, the “doors closed” light may still illuminate!
RAIB’s reconstruction of the incident showed that when the driver made the first CCTV check the intended passenger could have been masked from view by the ticket machine.
Mistaken reliance on the door interlock system was also a factor in a December 2017 incident at Radford Road, Nottingham, when a pushchair was trapped and dragged. RAIB has also previously investigated similar occurrences in Croydon, Bury near Manchester and Wood Street in northeast London.
Trams and train doors have obstruction detection devices, but they only detect objects that are 30mm or more in diameter. A fact that should be more widely publicised. The frequency of trapped and dragged incidents also deserves more attention. Is it reasonable to expect light rail, tram, metro, and indeed drivers of local trains to make multiple checks using CCTV before moving off?
There has to be a better way.
Near miss at Paddington Subway Junction
At 01:17 on the morning of 18 July, two trackworkers at Paddington Subway Junction in London were involved in a very near miss. The RAIB news story says they were facing away from the approaching train but moved clear with just “one or two seconds to spare”. It adds that the train was travelling at a mere 24mph when the near miss occurred. RAIB has decided to issue a Safety Digest. From my own experiences I recall the fatigue which is often experienced in the very early hours of the day.
Near miss at Penkridge
A week earlier on 11 July, a very near miss involving two trackworkers occurred at Penkridge in Staffordshire at six minutes after midnight. The trackworkers were investigating an overhead line fault that was preventing the use of electric traction, causing the disruption of train services. They were almost struck by a freight train travelling at 61mph just south of Penkridge station, Staffordshire. The track workers moved clear of the path of the train less than one second before it reached their position. Another train was passing the track workers on an adjacent line as the freight train approached them.
RAIB has begun its investigation which will consider “the actions of those involved, arrangements to protect trackworkers from moving trains, rules and responsibilities, working patterns of relevant staff, how competence of staff was managed, and relevant underlying factors”.
BESRs not implemented.
A new pneumonic (at least new to me) has entered the railway jargon dictionary – BESRs which refers to the imposition of Blanket Emergency Speed Restrictions. RAIB is investigating a number of instances of over speeding between 18-19 July, which occurred despite the imposition of BESRs due to the accurate forecast of extremely hot weather.
The RAIB website shows the eye-catching design of the notices that were produced for train operators and their drivers.
It has identified two incidents of over speeding on the Western Route on 18 July and two more incidents that occurred in Wales on 19 July. Despite the clarity of its notices, RAIB has said that “drivers had not clearly understood the BESR’s”.
The RAIB has decided to issue a Safety Digest. My expectation is that their focus will include the management supervision and methods used by driver management as well as the understanding of BESR’s by drivers. It will be interesting to read just how the train operating companies attempted to contact and instruct their drivers about the BESRs.

Wrong electrical section switched off
On 13 September, Network Rail’s Safety Central website issued a Safety Advice following an incident which could have resulted in fatalities. There has been a delay in publication as the incident occurred back on 1 June. Off Track and OLE staff from the Ipswich Delivery Unit were on site at Arlesford clearing vegetation that was overhanging the return conductor. They had a Safe Work Pack and it had been determined that an ‘OLE switch off’ (not an earthed isolation) was needed due to the proximity of the vegetation to the live OLE.
The switch off was taken by the Nominated Person and the Off Track team then started to clear overhanging branches. One of the branches fell onto the overhead lines resulting in two team members receiving electric shocks. An incorrect electrical section for the electrical switch off had been requested, so the work area OLE was live. In addition, approved isolated tools were not being used. Two team members attended A&E but were uninjured.
Prohibition notice
Network Rail’s Safety Central website issued a Safety Bulletin issued on 27 September following a visit by ORR inspectors that resulted in a prohibition notice.
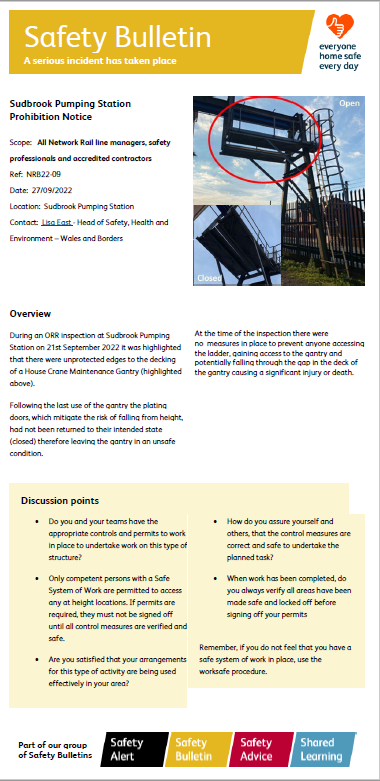
During the ORR inspection on 2 September, unprotected edges to the decking of a house crane maintenance gantry resulted in a prohibition notice being issued. The plating doors had been removed and not replaced, leaving the gantry in an “unsafe condition”. At the time of the inspection there was nothing in place to prevent anyone accessing the ladder and gantry or “falling through the gap in the deck of the gantry causing a significant injury or death.”
Improvement notices
I welcome the publication of the ORR’s annual review of Network Rail’s stakeholder engagement for 2021/22. Sixty percent of those surveyed gave a “good” rating – a drop of 13% compared to the previous year. To date this year six improvement notices have been served. They include: failing to provide adequate welfare facilities of drivers and conductors; failing to take sufficient precautions securing unbraked railway vehicles; and failing to make sufficient risk assessments for the health and safety of employees working at the Hilton Level crossing and Hartlebury Station. ORR also found failings in the review of risk assessments for railway operatives under the control of Eurotunnel.
Writing about all of these unfortunate events convinces me that much more needs to be done to improve safety. How many close calls or near misses will there be before someone is badly hurt or worse? The six ORR improvement notices may, by some of us, seem to be a very restrained response to the continuation of unsafe working.
